


Carbohydrate Digestion and Absorption
*This content has been reviewed by Dr. David Kitts (Faculty of Land and Food Systems, University of British Columbia)
Dietary carbohydrates include starches, sugars, and fibre.
- Use of Dietary Carbohydrates as Energy. Glucose is the primary energy source of the body. Major dietary sources of glucose include starches and sugars.
- Digestion of Carbohydrates. Dietary carbohydrates are digested to glucose, fructose and/or galactose, and absorbed into the blood in the small intestine.The digestion and absorption of dietary carbohydrates can be influenced by many factors.
- Absorption of Carbohydrates. Absorbed carbohydrate molecules are used immediately for energy or stored in various forms in the muscles, liver or adipose tissue for future use.
Use of Dietary Carbohydrates as Energy
Dietary carbohydrates include starches, sugars and fibre that are mostly found in grain products, vegetables and fruit, milk products, and meat alternatives such as nuts, seeds, and legumes (1, 2). Starches and sugars are the major dietary sources of glucose, which is the primary energy source in the body:
- The brain relies primarily on glucose to function; restricting the brain’s glucose supply can impair memory and ability to focus.
- Muscles use glucose for energy, especially during high-intensity exercise.
 Digestion of Carbohydrates
Digestion of Carbohydrates
Before the body can use the food that is eaten, it must be “digested” (i.e. broken down) into its basic nutrient components.
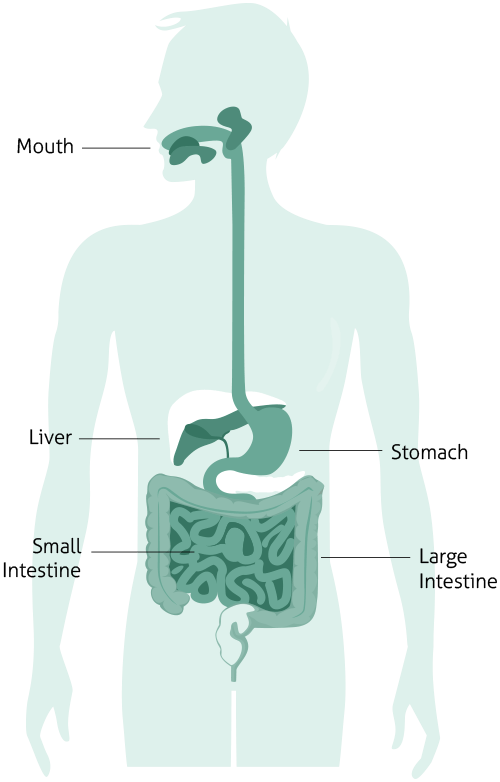
The digestive system works like a giant food processor. During digestion, starches and sugars are broken down both mechanically (e.g. through chewing) and chemically (e.g. by enzymes) into the single units glucose, fructose, and/or galactose, which are absorbed into the blood stream and transported for use as energy throughout the body.
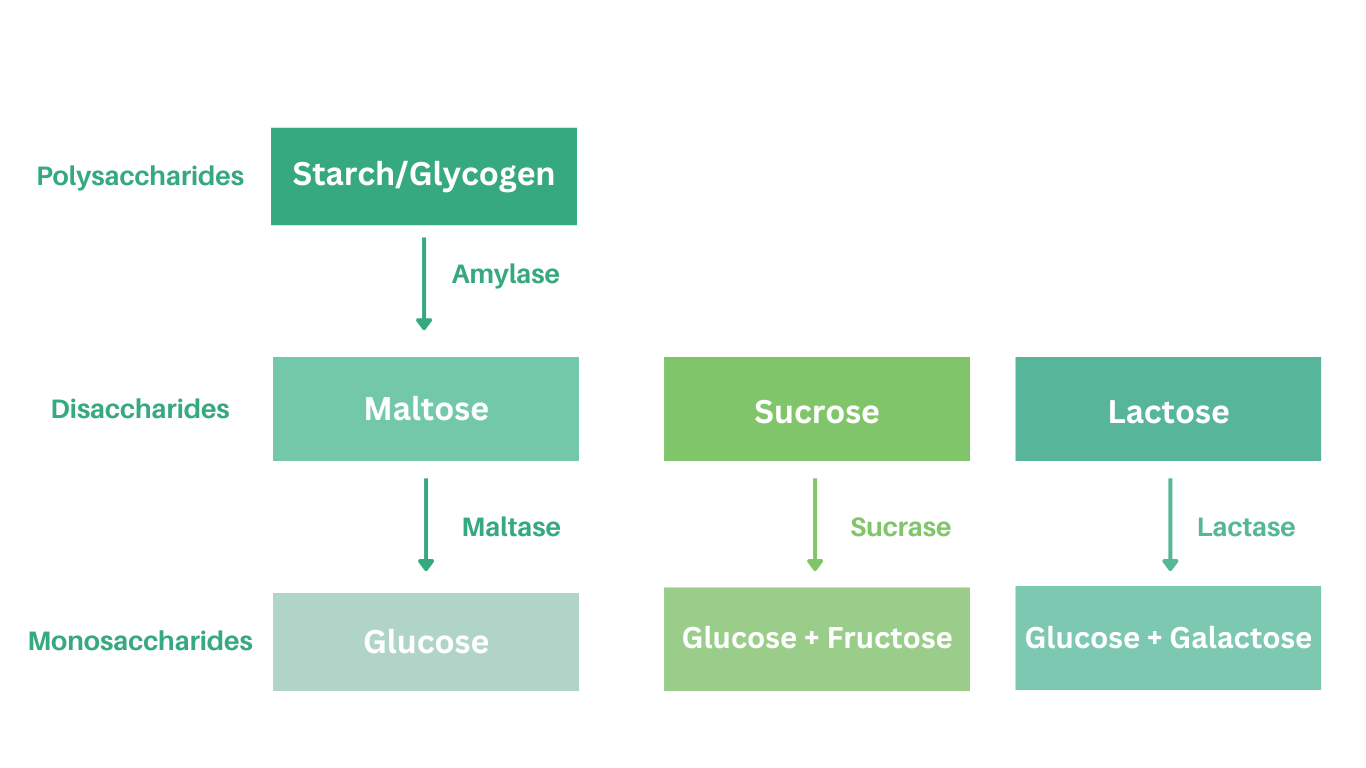
Digestion of starches into glucose molecules starts in the mouth, but primarily takes place in the small intestine by the action of specific enzymes secreted from the pancreas (e.g. α-amylase and α-glucosidase). Similarly, the disaccharides sucrose, lactose, and maltose are also broken down into single units by specific enzymes (See table below) (3, 4).
Absorption of Carbohydrates
The end products of sugars and starches digestion are the monosaccharides glucose, fructose, and galactose. Glucose, fructose, and galactose are absorbed across the membrane of the small intestine and transported to the liver where they are either used by the liver, or further distributed to the rest of the body (3, 4).
Absorption of Fructose
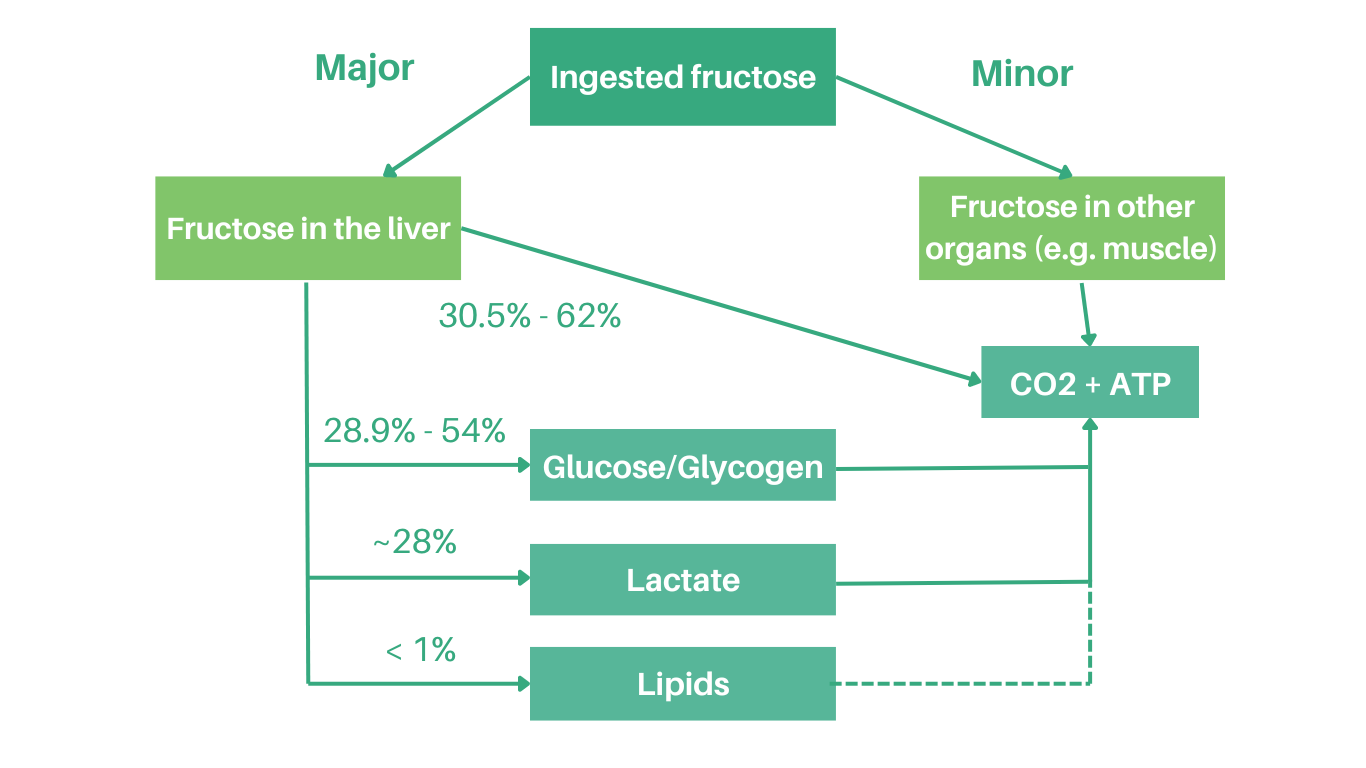
There are two major pathways for the metabolism of fructose (5, 6): the more prominent pathway is in the liver and the other occurs in skeletal muscle. The breakdown of fructose in skeletal muscle is similar to glucose. In the liver and depending on exercise condition, gender, health status and the availability of other energy sources (e.g. glucose), the majority of fructose is used for energy production, or can be enzymatically converted to glucose and then potentially glycogen, or is converted to lactic acid (See figure below).
The notion that fructose is an unregulated energy substrate and directly fuels fat synthesis in the liver is not supported by the scientific literature; within the normal consumption range very minimal amounts (<1%) of fructose are converted to fat (5, 6). It is important to note that the metabolism of fructose involves many regulated reactions and its fate may vary depending on nutrients consumed simultaneously with fructose (e.g. glucose) as well as the energy status of the body.
Figure. Acute metabolic fate of fructose in the body within 6 hours of ingesting 50-150 grams (about 12-36 teaspoons) of fructose (adapted from Sun et al., 2012)
Factors that Affect Absorption of Carbohydrates
A number of factors affect carbohydrate digestion and absorption, such as the food matrix and other foods eaten at the same time (7).
Glycemic Index (GI) is a scale that uses a numbering system to rank carbohydrate rich foods as “high GI”, “medium GI”, and “low GI” based on the rate that glucose-containing carbohydrates are digested and absorbed, and the rate they increase blood glucose levels (8, 9). Foods with a high GI are more quickly digested, and cause a larger increase in blood glucose level compared to foods with a low GI. Foods with a low GI are digested more slowly and do not raise blood glucose as high, or as quickly, as high GI foods. Examples of factors that affect carbohydrate absorption are described in the table below:
| Factors that Affect Carbohydrate Absorption | Examples |
|---|---|
| Cooking: Foods that are less cooked or processed are digested more slowly and have a lower GI than foods that are more cooked or processed. |
Less processed foods, such as slow cooking oats or brown rice, have a lower GI than more processed foods such as instant oats or instant rice. Pasta cooked 'al dente' (tender yet firm) has a lower GI than pasta cooked until very tender. |
| Fibre: Fibre helps to slow digestion of carbohydrate foods. High-fibre foods tend to have a lower GI than low fibre foods. | High fibre foods such as whole grain breads, oats, beans, and lentils, have a lower GI than low fibre foods such as white bread and rice cereal. |
| Fat and Protein: Fat or protein eaten along with carbohydrate helps to slow down digestion and reduces the GI of carbohydrate. | A snack that includes carbohydrate with protein or fat has a lower GI than a snack with carbohydrate only. For example, crackers with peanut butter have a lower GI than crackers alone. |
| Acids in Foods: Acids in foods slow the time it takes for the stomach to empty after eating. Acids lower the GI of carbohydrate foods. | Vinegar, lemon juice, or citrus fruits added to foods will lower the GI of those foods. |
For more information, additional resources include:
- Clips on Sugars - Understanding the Glycemic Index
- Carbohydrate News - Sugars and Health: The Current Science
- Video - Sugar 101: Journey of a Sucrose Molecule
References
- Report of a Joint FAO/WHO Consultation. Carbohydrates in Human Nutrition. Rome, IT: Food and Agriculture Organization of the United Nations; 1998.
- Cumming JH, Stephen AM. Carbohydrate Terminology and Classification. Eur J Clin Nutr. 2007;61(Suppl1):S5-S18.
- Southgate DA. Digestion and metabolism of sugars. Am J Clin Nutr. 1995;62(Suppl):203S-11S.
- Levin RJ. Digestion and absorption of carbohydrates – from molecules and membranes to humans. Am J Clin Nutr. 1994;59:690S-98S.
- Tappy L, Le K. Metabolic effects of fructose and the worldwide increase in obesity. Physiol Rev. 2010;90:23-46.
- Sun SZ, Empie MW. Fructose metabolism in humans-what isotopic tracer studies tell us. Nutr Metabol. 2012;9:89-103.
- Anderson GH, Woodend D. Consumption of sugars and the regulation of short-term satiety and food intake. Am J Clin Nutr. 2003 Oct;78(4):843S-849S.
- Diabetes Canada. The Glycemic Index [Internet]. Diabetes Canada; 2024 [cited 2024 Mar 1].
- Canadian Sugar Institute. The Glycemic Index: Clinical and Public Health Significance [Internet]. Canadian Sugar Institute; 2008 [cited 2024 Mar 1].